Part of our complete guide to Ptosis (Droopy Eyelid) — this page covers ptosis treatment and surgery in depth.
Treatment of Ptosis
The choice of operation depends on three factors: the degree of ptosis, the remaining levator function, and the phenylephrine test result. Dr. Riske reviews all options with you at consultation and tailors the approach to your anatomy and goals.
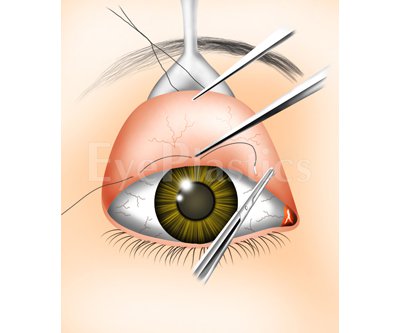
Incision made through the inner conjunctival surface of the lid — no external scar
Best candidates: good levator function (≥ 10 mm) and a positive phenylephrine test
The amount of Müller muscle and conjunctiva resected is determined by a formula based on the phenylephrine response
Typically performed under local anesthesia with light sedation; because the resection amount is set by the phenylephrine-based formula, no awake intraoperative adjustment is required
Can be combined with cosmetic upper blepharoplasty
Levator Advancement (External Approach)
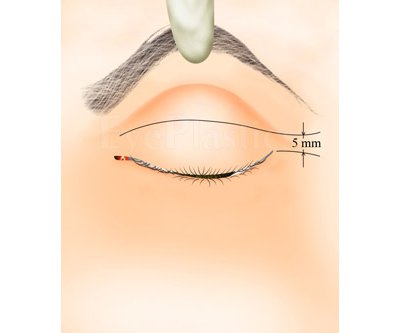
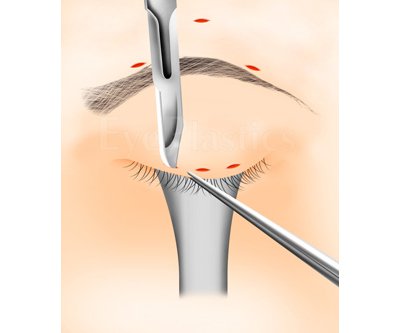
Incision placed within the upper lid crease — scar is hidden in the natural skin fold
The aponeurosis is reattached or tightened to the tarsus under direct vision
Patient is awake during the key adjustment step so lid height and contour can be refined in real time
Preferred for aponeurotic ptosis with moderate-to-good levator function
Can be combined with cosmetic upper blepharoplasty through the same incision
Frontalis Sling
The eyelid is suspended directly from the frontalis (forehead) muscle using a sling material
Required for severe ptosis with poor levator function (≤ 4 mm) — the typical situation in congenital ptosis and Marcus Gunn jaw wink. Congenital ptosis carries roughly a 30% risk of amblyopia (from lid occlusion or induced astigmatism), so affected children need prompt pediatric ophthalmology evaluation
Sling materials include autogenous fascia lata (harvested from the thigh), silicone rod, or Gore-Tex
The patient opens their eye by raising their brow, not by contracting the levator
Some lid lag on downgaze and lagophthalmos (incomplete lid closure on attempted closure and during sleep) are expected; lubricating eye drops/ointment are needed long-term
Performed under general anesthesia; lid height is determined by a surgical formula
Ptosis Surgical RepairInteractive Animation
Explore eyelid anatomy and the three main ptosis repair techniques: Internal, External, and Frontalis Sling.
Ptosis Surgical RepairInteractive Animation
Choose an approach, then drag the slider to step through it.
Anatomy — drag the slider to step through.
In the results below, note how the lid margin rises off the pupil to a natural height and the eyelid crease becomes visible again. A well-executed repair restores symmetry with the other eye — the goal is a rested, open appearance, not a surprised one.
Fasanella-Servat Procedure
For mild ptosis with good levator function, the Fasanella-Servat procedure removes a small strip of the upper tarsus, Müller’s muscle, and conjunctiva from the back of the lid. It is quick and predictable for small (1–2 mm) corrections and leaves no external incision.
Frontalis Sling Materials
When levator function is poor (often in congenital ptosis), a frontalis sling links the lid to the brow. Materials include autologous fascia lata (harvested from the thigh — the most durable, preferred in older children and adults) and synthetic options such as silicone, Gore-Tex (ePTFE), Supramid, or Mersilene mesh, which allow earlier surgery in young children.
Ptosis RepairBefore & After
Before-and-after results, one case at a time.
Age 45 — before and after ptosis repair
Upneeq®
Upneeq® (oxymetazoline hydrochloride ophthalmic solution 0.1%) is the first and only FDA-approved prescription eye drop for acquired low-lying eyelids in adults. It is a non-surgical option for patients with mild ptosis.
How It Works
Oxymetazoline is an α-adrenergic agonist that selectively stimulates Müller’s muscle, lifting the upper eyelid by approximately 1 mm within 5 minutes of instillation. The effect lasts up to 8 hours.
Key Facts
Once-daily drop applied to each ptotic eye
Single-use, preservative-free container; discard after each dose
Contact lenses must be removed before instillation; may be reinserted 15 minutes later
Average eyelid lift is ≈ 1 mm — meaningful for mild ptosis; not sufficient for moderate or severe ptosis
Clinical trials showed statistically significant improvement in superior visual field at 2 and 6 hours post-dose
Who Is a Candidate
Adults with mild acquired aponeurotic ptosis who prefer a non-surgical option
Patients who show lid elevation on the phenylephrine test
Patients who are not yet surgical candidates due to other health conditions
Precautions
Use with caution in patients with cardiovascular disease, uncontrolled hypertension or hypotension, or orthostatic hypotension — alpha-agonists affect vascular tone
May increase the risk of angle closure glaucoma in patients with untreated narrow-angle glaucoma
New ptosis with a variable or fatigable pattern (suggesting Myasthenia Gravis), or with a dilated unreactive pupil, requires specialist evaluation before Upneeq is prescribed
Ptosis Repair Before & After
1 / 6
Drag the divider left or right to compare. Select a case in the strip below.
BeforeAfter
Age 53Patients are from a national database. Individual results may vary.
Frequently Asked Questions
Which ptosis operation will I need?
It depends on levator function and the phenylephrine response. Good function with a positive phenylephrine test often allows an internal Müller's-muscle resection; weaker function calls for external levator advancement; very poor function is treated with a frontalis sling.
Is ptosis surgery covered by insurance?
Usually, when the droop obstructs vision — documented with a visual-field test and photographs. Purely cosmetic lifts are out-of-pocket.
What is Upneeq?
Upneeq (oxymetazoline 0.1%) is a once-daily prescription eye drop that temporarily lifts the upper lid by stimulating Müller's muscle — a non-surgical option for mild, acquired ptosis.